
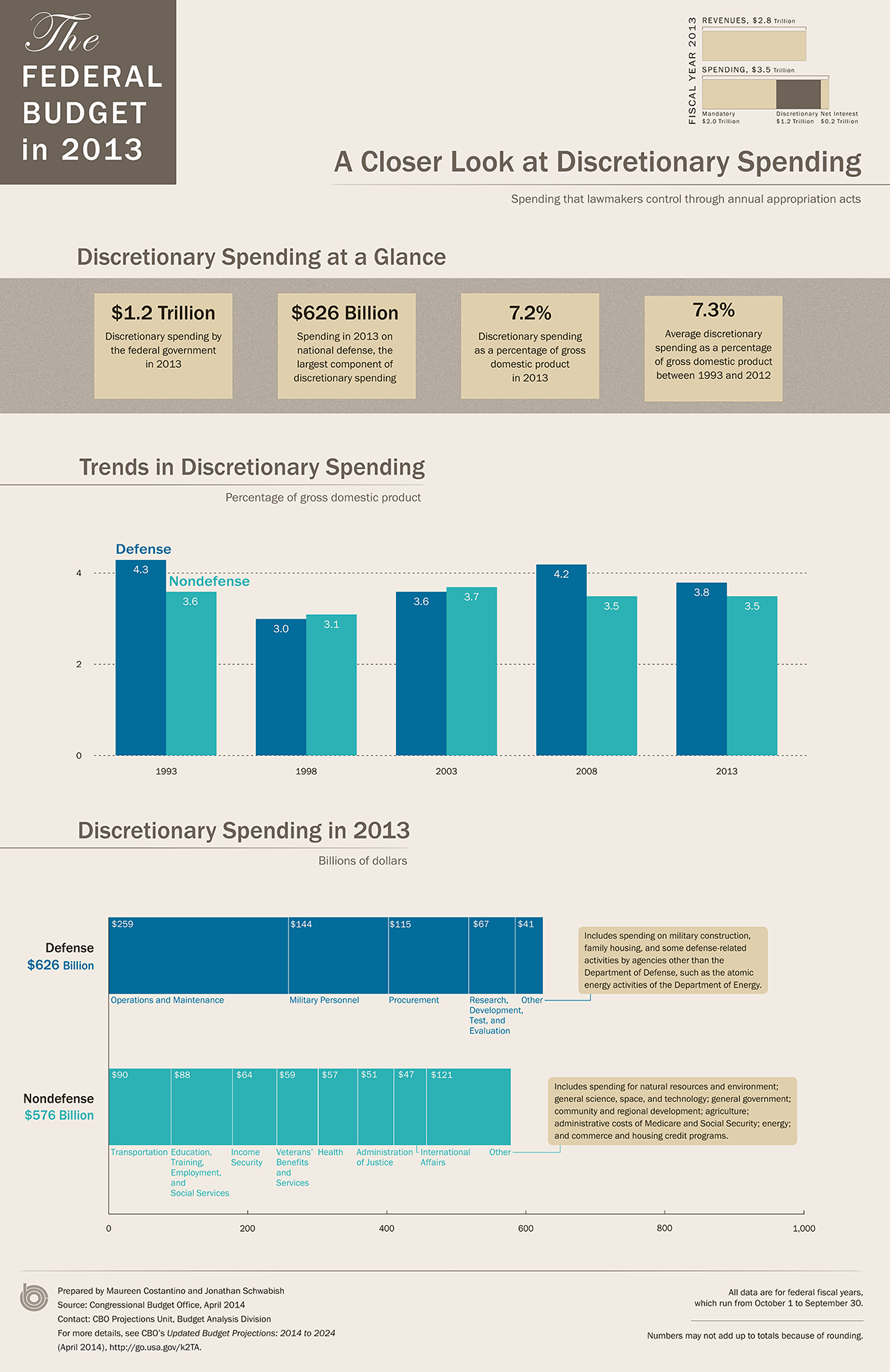
CBO projections about federal discretionary spending. Most of the dollars for the Indian health system come from this category. LARGE VERSION
I like asking questions about the big picture: What does the Indian health system look like a year from now? What about in a decade? Or even longer? The answers might be found deep within the pages of budgets; line by line predictions about the future. Let’s start with good news: The cost of diabetes treatment is declining in Indian Country. Ever. So. Slightly. Still, that ought to be both celebrated and reason enough to look deeper at what’s working and explore what more can be done. The Special Diabetes Program for Indians has more than doubled the number of grants to health care providers and invested in community-designed solutions. The result is that End Stage Renal Disease fell by nearly 40 percent from 1995 to 2011 — a greater decline than any other racial or ethnic group. “Given that the Medicare cost per year for one patient on hemodialysis was $82,285 in 2009, this reduction in the rate of new cases of ESRD means a decrease in the number of patients who would have required dialysis— translating into millions of dollars in cost savings for Medicare, IHS, and other third-party payers, as well as improved quality of life for patients who do not need dialysis,” according to testimony by Dr. Yvette Roubideaux, acting IHS director, to the Senate Committee on Indian Affairs last month. “Diabetes health outcomes have also improved significantly in American Indian and Alaska Native communities since the inception of the SDPI. One of the most important improvements has been a 10 percent reduction in the average Hemoglobin A1C levels of American Indians and Alaska Natives with diagnosed diabetes. Improved blood sugar control contributes to reductions in complications from diabetes.” Why does that matter? Every percentage point drop in A1C results in reduced risk of eye, kidney, and nerve complications by some 40 percent. Even Congress could not ignore such a cost effective success story. But instead of a three-year authorization, the smart path, Congress could only muster enough support for a single year extension. When a program that saves lives and money cannot win approval beyond a year, well, that’s evidence about the broken nature of the funding mechanism. Then, there are so many examples of cost-effective health care delivery that could save money (and improve service), such as funding Indian health budgets in advance, limiting payments to outside providers based on Medicare rates, or expanding mid-level dental providers. All “to do” items for that magical day when Congress is more interested in solving problems than being a forum for slogans about cutting spending. And that’s what’s frustrating. Neither the Congress nor the Obama administration is investing enough in the areas of the budget that will reduce future costs or add additional revenue. The problem is the Indian health system is at risk from the congressional appropriations process. Over the next decade this category of spending is shrinking. The administration is encouraging American Indians and Alaska Natives to sign up for insurance programs under the Affordable Care Act. The Indian Health Service estimates third-party collections to increase to $1.2 billion over the next year, including an additional $22 million in Medicaid. That’s realistic. But given the long term challenges in the appropriations process, should this not be a stretch goal? What if there were a national campaign (with real-time data) for American Indians and Alaska Natives to reach lofty insurance targets? One tribe that’s doing just that is Jamestown S'Klallam in Washington. The tribe’s web page is blunt, telling tribal members that they “must” sign up for Medicaid when eligible. Same goes for private insurance. “If you are eligible for free insurance coverage through your employer, spouse’s employer or another entity, you must sign up for the coverage and use it,” says the tribe’s Health and Human Services. And if a member is not eligible for any other program, then, as a last resort, then a basic health plan is purchased for members. Perhaps no tribe will ever get to 100 percent coverage, but what 95 percent? Possible. Do-able. This goes well beyond the “mandatory” coverage requirements in the Affordable Care Act. Then I bet it will be cost effective for the tribe because it’s creating a full-funding lever through insurance. This is the opportunity for Indian Country and the Indian health system. The Kaiser Family Foundation estimates that nearly one in three American Indians and Alaska Natives are uninsured. So what if that number were measured, reported, and reduced to one-in-five? Or better. As a Kaiser policy brief states: “Although the IHS budget has increased over time, funds are not equally distributed across facilities and they remain insufficient to meet health care needs. As such, access to services through IHS varies significantly across locations, and American Indians and Alaska Natives who rely solely on IHS for care often lack access to needed care. Moreover, as a discretionary program IHS funding is subject to the automatic funding cutbacks under the sequester, which further limit access to services.” The big picture is that Medicaid and insurance, automatic funding mechanisms, are the future. All budgets should reflect that. I still think that means taking Medicaid management away from the states for the Indian health system. Remember more than half of the uninsured population of American Indians and Alaska Natives live in states without Medicaid expansion. So that means patients in Washington could have far better access to medical treatment, especially purchased care, than a patient in Oklahoma. That’s not fair and needs to be resolved. Now back to the budget mess that is Congress. The budget deal between Sen. Patty Murray and Rep. Paul Ryan is temporary relief. It’s enough money to prevent damage to the Indian health system, but not nearly enough to carry out the work. It’s the opposite of cost effective. That said: Budgets are going to get far worse soon. Budget Control Act levels return in 2016 with new rounds of sequester and misery. The Congressional Budget Office estimates that appropriations will shrink from 7.2 percent of the economy in 2013 to only 5.1 percent by 2024. (Appropriations are already below average spending levels, and the lowest since World War II.) The ideal, of course, would be for friends of Indian Country to enact a special budget that puts treaty obligations ahead of everything else and funds the Indian Health Service at levels that compare to every other health care delivery system. That would be a leap since current appropriations only reach about 56 percent of its need, according to testimony from the National Congress of American Indians. “In 2012, IHS per capita expenditures for patient health services were just $2,896, compared to $7,535 per person for health care spending.” Full funding for Indian health is a nice ideal. But for money to be appropriated at levels even close to parity, Congress would have to do something that’s never been done before in the history of the United States. And, at a time when there are not even enough votes to invest more time and money in a diabetes initiative that is exceeding expectations. So what does the Indian health system look like a decade from now? The answer depends on how quickly individual American Indians and Alaska Natives get health insurance, funding that’s automatic. The alternative is Indian health budgets that shrink beyond recognition. Mark Trahant is the 20th Atwood Chair at the University of Alaska Anchorage. He is a journalist, speaker and Twitter poet and is a member of the Shoshone-Bannock Tribes. Join the discussion about austerity. Comment on Facebook at: www.facebook.com/TrahantReports More from Mark Trahant:
Mark Trahant: Dueling budget proposals impact Indian programs (04/09)
Join the Conversation

{kind=link}