A new report reveals that chronic understaffing at the Indian Health Service denies patients quality care.
By Elena Saavedra Buckley
High Country News
HCN.org
Almost a quarter of all positions for physicians, nurses and other care providers at Indian Health Service (IHS) facilities are vacant in most service regions, according to a
report published in August by the Government Accountability Office, or GAO. This prevents the agency from providing “quality and timely” health care to tribal citizens.
Established in 1955 to provide direct care to enrolled members of 573 federally recognized tribes, IHS operates a network of 55 health centers, 26 hospitals and 21 health stations, primarily in rural areas. In 2016, those facilities received 5.2 million outpatient visits and admitted more than 15,000 inpatients. In 2016, approximately $1.9 billion was allocated to fund these services.
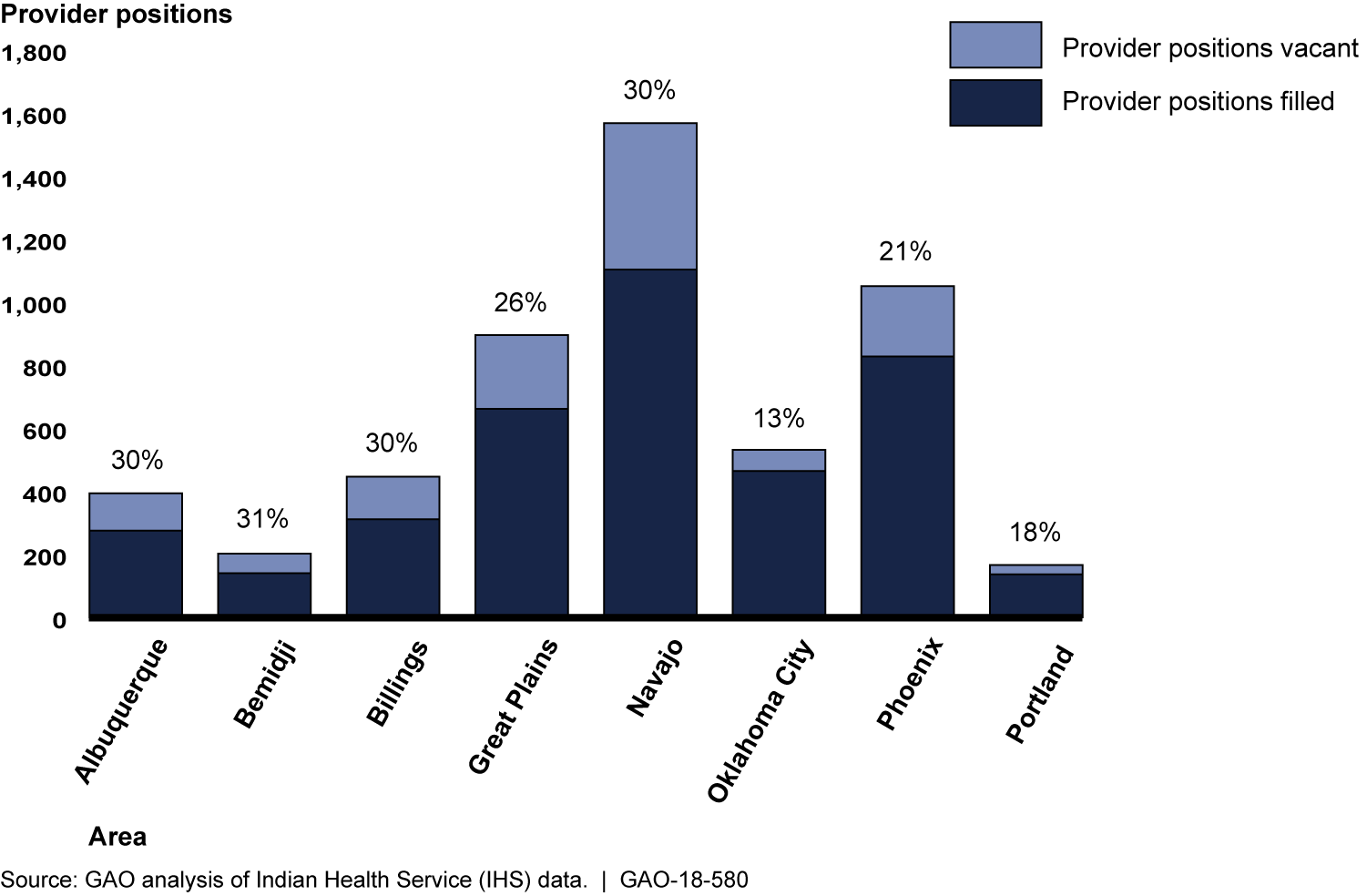 In half of IHS's coverage areas, a third of health care provider positions sit vacant.
Source: GAO analysis of November 2017 IHS data / GAO-18-580
In half of IHS's coverage areas, a third of health care provider positions sit vacant.
Source: GAO analysis of November 2017 IHS data / GAO-18-580
The GAO report looked at eight geographical areas and found that between 13 and 31 percent of provider positions were currently vacant. Many patients receive curtailed services as a result. “One doctor we spoke with,” read the report, “described this dynamic of vacancies begetting additional vacancies as a ‘never-ending cycle.’”
Many IHS facilities, often in rural areas and on reservations, are considered “isolated hardship” sites, designated as “unusually difficult” posts for providers. The problem frequently stems from an inability to provide market salaries or housing for providers. Even incentive programs, like student loan repayment in exchange for service contracts, lack funding. In the Billings area, for instance, five physicians left IHS in a two-week period after they failed to receive loan repayments. Many facilities must rely on short-term employees, even though the practice is often more costly than hiring full-time staff.
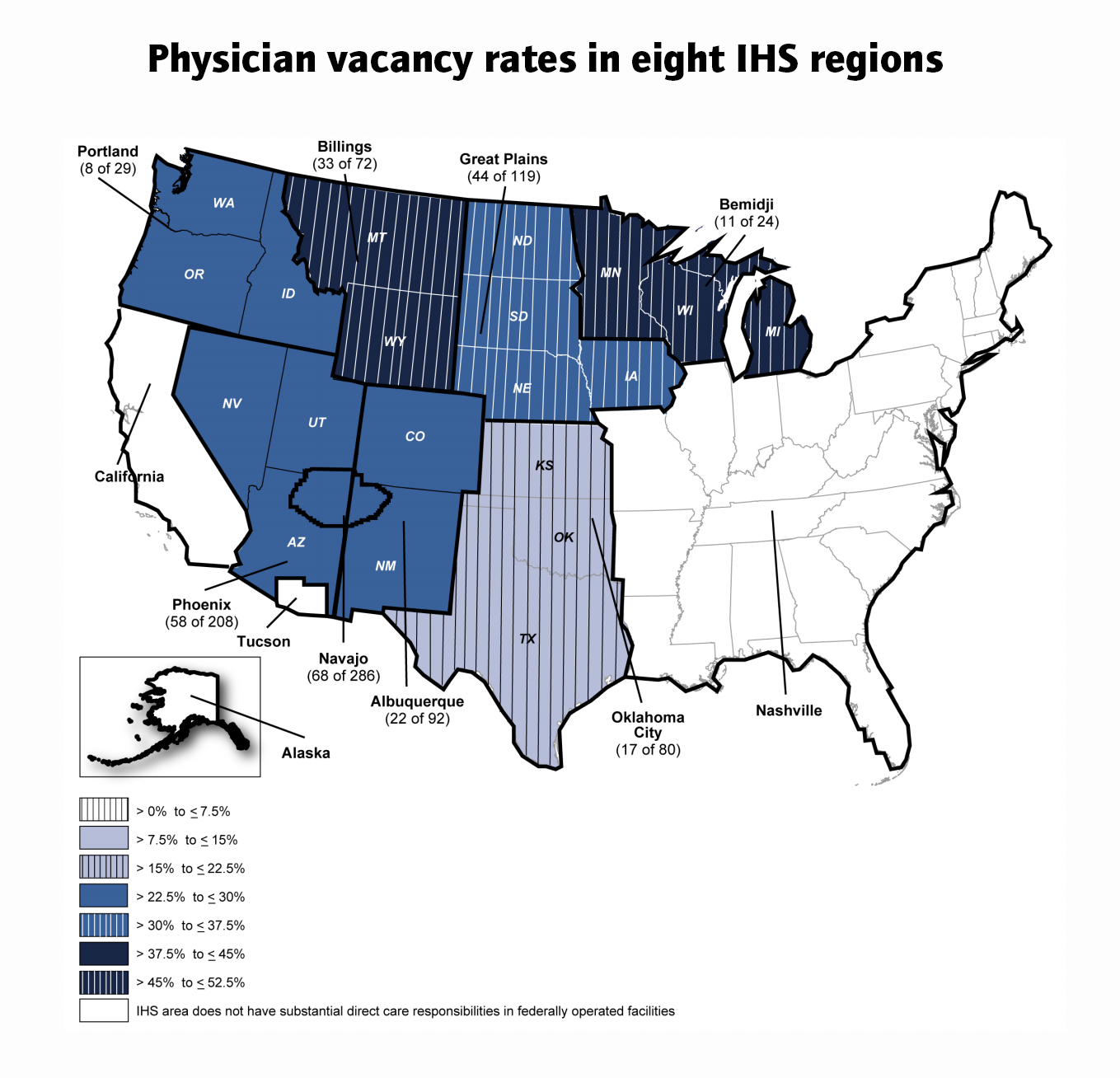 Physician vacancy rates are even higher, with some regions filling only half of their desired positions. Source: GAO analysis of November 2017 IHS data / GAO-18-580
Physician vacancy rates are even higher, with some regions filling only half of their desired positions. Source: GAO analysis of November 2017 IHS data / GAO-18-580
Some clinics and hospitals have had to cut services. At the Nevada Skies Youth Wellness Center, a substance abuse treatment facility for adolescents, staff shortages led to a decrease in the number of beds available. At a hospital in Rosebud, South Dakota, OB/GYN patients have been diverted to facilities 45 miles away since 2016. Chlamydia tests at the San Sioux Hospital, also in South Dakota, had to be sent to other laboratories, sometimes delaying treatment for over a week. In 2016, the National Congress of American Indians estimated that IHS allocates $2,849 per patient, compared to $7,717 per person for health-care spending nationally.
The GAO report recommends that the IHS director obtain more information on temporary employee contracts in order to make better decisions on the agency’s budget.
The government-to-government relationship between tribes and the United States sets the legal basis for providing American Indian and Alaska Natives with health care. In exchange for land cessions, the federal government promised to provide assistance for Indigenous people, including medical services.
Elena Saavedra Buckley is an editorial intern at High Country News. Follow
her on Twitter @elenaSB_
This story was originally published at High Country News (
hcn.org) on
October
8, 2018.
Government Accountability Office Report
Indian Health Service:
Agency Faces Ongoing Challenges Filling Provider Vacancies (August 15, 2018)
Join the Conversation
Related Stories
Indian
Health Service still seeing high vacancy rates (August 22, 2018)

